


Covid: The End of Hope Hypothesis (part three)
Integrating everything to (in)validate the hypothesis

Ways to validate the hypothesis
There are three ways to validate the hypothesis, two of which could be considered non-technical or non-specialist.
Linguistic validation: do the terms used in the hypothesis make sense in context and are they sufficiently correctly or coherently used? For example, “discombobulation of LINE-1 phagocytes leading to reverse mutations in CDKN1B” would be an easily identifiable and verifiable load of probable BS, on which basis I would throw out the hypothesis on linguistic grounds.
Logical validation: based on what we presently know about the hypothesis’ components and wider relevant phenomena, does the hypothesis hang together in a logical sense?
Technical validation: This is where varying degrees of specialist knowledge come into play in evaluating what are clearly technical claims put forwards in the hypothesis. This will be beyond most non-specialists.
What I have provided up to this point does not completely validate the hypothesis. I will make this clear where appropriate.
The End of Hope hypothesis, step-by-step
Step 1
1 . Make mRNA coding for S protein
This has already been done. The vaccines have achieved this.
Step 2
2. Make mRNA coding for mutant versions of CYP19A1 and CDKN1B in smaller amounts
Linguistically, what this step means is that another exogenous, synthetic “mRNA” payload is delivered via the “vaccines” that results in the host organism being triggered, somehow, to then “manufacture” mutated versions of these two genes that both have meaningful, likely persistent, effects on the host. At a stretch, this could be interpreted as the payload directly mutating those genes in a given cell’s DNA helix, but that’s pushing the language further than I would tolerate, because the specificity of the terms and their implications are important. Given the complexity of mutating specific genes exogenously, I think that the shortness of this step combined with flaws in the use of terms makes it suspect.
On this basis, I have doubts about the validity of this step. messenger RNA is the result of gene expression, that is the readable code for protein production by the ribosome, in the context of what is supposed to be going on with Covid gene therapies.
However, there is something else that until now, I was unaware of but my knowledge is practically zero. Read the whole short page via the link.
January 2020:
Modified RNA is distinct from messenger RNA, which simply comprises instructions for building proteins; messenger RNA, the basis of two prominent COVID vaccines, does not affect DNA.
Following a new collaboration between UiO and research groups in Nottingham and Oxford, it has now been revealed that RNA has a direct effect on DNA stability, according to Professor Klungland's research.
He believes the discovery will provide the health service with an important tool, since many studies have shown that the regulation of modifications to RNA is important for the development of cancer.
The referenced paper is behind a paywall.
Logically, I am ambivalent about this, but that could be due to lack of knowledge. mRNA, to my knowledge, doesn’t modify genes according to the claims of the manufacturers. But, the evidence of possible reverse transcription capability of the Pfizer vaccine suggests that in some human cell types and under some circumstances, mRNA itself might enter the cell nucleus and write into human DNA with some unknown purpose or function. If that is true and it is a real, hidden capability, then logically, there’s a possibility that DNA is modified somehow. Whether such modifications can directly target two specific genes and thereby mutate them is more a technical question than logical one.
Technically, [EDIT] There was no regulator/manufacturer research into any mutagenic effects in humans and no published official research on the content of any batches in production. This means that if there is an effect on these two genes, no one has investigated it in a way that could have affected approval/rollout.
As of April 2023, independent research has demonstrated:
LINE-1 RT capability in vitro in human liver cells.
Contamination of Covid gene therapies with out of spec mRNA and DNA material, the function/effect of which is unknown, despite being deliberately limited by regulators without explanation #plasmidgate.
genetic sequences of Covid gene therapies by independent researchers is underway.
Step 3
[EDIT] Corrections made to include female gonads references.
3. Make sure that while delivery system for (1) mostly ends up in liver, most of (2) ends up in the gonads
Linguistically, this step states that the vaccines can mechanistically target different tissues or organs and thereby take two different payloads to two different organs. So, the Spike-encoding mRNA payload in its LNP wrapper has a determinedly greater affinity for and probability of aggregating in the liver, both by the LNP’s properties and how the body processes them. Likewise, if there is this second payload targeting two specific genes, the LNP wrapper in use there has some greater affinity for and probability of ending up in the gonads. This step makes no claims about the relative proportions of either payload in a dose.
Logically, I think this could be possible, depending upon what the real capabilities of LNP wrappers really are. It’s logically possible to have some kind of characteristic or property that results in a possible tissue type affinity, but there remains a question of how that would be achieved and how biological factors would affect the biodistribution. Also, logically one could ponder whether an external factor could come into play in helping the payload get predominantly to the gonads. Using a bit of knowledge and imagination, I’ll throw out a theory to illustrate, logically, how this could be done.
If one researches the concept of biomagnetism, for example, one will find extensive research going back years into the use of ferrous LNPs as injectable wrappers for bioactive payloads. Once inside the body, the use of a magnetic field can draw those LNPs to a location where the magnetic field is applied. Thus, the payload can be delivered to a specific zone of the body.
In the case of male gonads, most men carry a mobile phone in their pockets near their gonads. If an LNP wrapper could be manufactured that had inductive properties that reacted with a mobile phone’s properties or transmissions, this could provide a means to effectively draw those LNPs into the pelvic region, thereby increasing the chances of LNP uptake in that region, which encapsulates the gonads.
It is now clear that LNPs can accrete in the gonads either by design or by virtue of their ability to move around the body and transfect any or many tissue types, including the gonads, seemingly irrespective of external mechanisms.
Technically, as of April 2023, it appears that this step is technically possible based on Pfizer’s own Japanese Biodistribution study in mice, as well as non-Covid LNP research that states LNPs can be specifically designed to have an affinity for cell types e.g. the placenta. Given that fertility studies in humans are sparse for Covid gene therapies, there seems to be little to no evidence ruling out this step as technically possible.
What Pfizer’s own animal pharmacokinetic study showed is that at 48-hours post injection 16% of its gene therapy LNPs accumulated in the liver, 0.74% in the testes and 0.095% in the ovaries. This liver aggregation is likely to be the natural result of the body’s processing and the transport of the LNPs via the blood and lymphatic systems into the liver. However, the published claims around these LNPs states that they are by design practically invisible to the immune system because they consist of lipids. Their predominant means of cell transfection hinges around, if I remember correctly, ionic pressure/charge differential. If the LNPs have time and ability to circulate through the body with roughly uniform ability to transfect any cell type, why is there such a liver-dominant aggregation?
Also, the trial pharmacokinetics study is Pfizer’s not Moderna’s and also there’s nothing to say that what was used in that study is truly reflective of what is being deployed in humans. The LNPs in that study weren’t the real production final formulation containing the mRNA payload and comprised Luciferase to aid detection. It could be easy to use a different formulation in some, many or all batches. howbadismybatch.com has the facility to compare the number of reported adverse events per batch number and the distribution of results show that about 5% of batches (last time I checked) were associated with the majority of reported adverse events.


Step 4
4. Make sure form and quantity of additive upregulating LINE-1 reverse transcription activity makes it hard to detect among legit adjuvants
Linguistically, there’s a few things going on here.
A specific additive is present that “upregulates LINE-1 RT activity”. What form that additive takes and how much is present makes hard to detect amongst the other ingredients (“adjuvants”).
An adjuvant is “an immunological agent that increases the antigenic response.” Adjuvants are typically present in non-mRNA/DNA based vaccines, and might include Alum or Thiomersal. Search the EMA Moderna Spikevax EPAR document for “adjuvant” and there are zero hits. Search for excipients and there are many.
An excipient is a substance formulated alongside the active ingredient of a medication,[1] included for the purpose of long-term stabilization, bulking up solid formulations that contain potent active ingredients in small amounts (thus often referred to as "bulking agents", "fillers", or "diluents"), or to confer a therapeutic enhancement on the active ingredient in the final dosage form, such as facilitating drug absorption,[2][3] reducing viscosity,[4] or enhancing solubility.[5] A comprehensive classification system based on structure-property-application relationships has been proposed for excipients used in parenteral medications.[6][7]
Often, more excipient is found in a final drug formulation than active ingredient, and practically all marketed drugs contain excipients.[1]: 1 As with new drug substances and dosage forms thereof, novel excipients themselves can be patented; sometimes, however, a particular formulation involving them is kept as a trade secret instead (if not easily reverse-engineered).
This Wikipedia page shows that adjuvants are a type of excipient.
In the case of Moderna’s Spikevax, its excipients include:
SM-102 Heptadecan-9-yl 8-((2-hydroxyethyl) (6-oxo-6-(undecyloxy) hexyl)
amino)octanoate (novel)
PEG2000-DMG 1,2-Dimyristoyl-rac-glycero-3-methylpolyoxyethylene (novel)
Cholesterol
DSPC 1,2-distearoyl-sn-glycero-3-phosphatidylcholine (novel)
Tromethamol, acetic acid, sodium acetate trihydrate, sucrose and water for injections
tromethamine hydrochloride
The EMA is essentially describing all ingredients of Spikevax as “excipients”, including sucrose and water.
If “adjuvants” are a subset of excipients, it’s linguistically possible that the author of the hypothesis lacked the specific knowledge or context to distinguish between the two, or that at the point the hypothesis was published, the term adjuvant was in use.
Is “LINE-1 reverse transcription activity” linguistically valid? Yes:
The specificity and flexibility of l1 reverse transcription priming at imperfect T-tracts
Here, we employed a direct assay for the initiation of L1 reverse transcription to define the molecular rules that guide this process.
However, reverse transcription and retrotransposition are different but related technical terms. A 1989 paper listed them as such:
Logically, this step hypothesizes that there is an additive present that increases/stimulates/upregulates LINE-1 reverse transcription activity. We’ve seen that there are multiple substances including drugs and proteins whose presence has a possible upregulating effect on LINE-1 retrotransposition.
Technically, depending upon the correct interpretation and use of the terms reverse transcription and retrotransposition, what this step is implying is:
Increasing LINE-1 activity via the presence of a deliberately stimulating additive is necessary to achieve some effect, related to one or both payloads.
Deliberately increasing LINE-1 activity, as seen in Part Two, can serve as an indicator of cancer, can modulate the immune system, is either associated with or causal of inflammatory and autoimmune responses, amongst other things. It’s possible that it could be a cause of cancer, although not definite from the references in cited.
The additive also serves a purpose of increasing dose effect (acting as an adjuvant), which is also something an excipient can do.
The form and amount of this additive can be deliberately controlled in such a way as to make it hard to detect.
We’ve seen research that suggests that the Pfizer gene therapy has the capability to reverse transcribe into human DNA. That mechanism involved LINE-1:
We detected high levels of BNT162b2 in Huh7 cells and changes in gene expression of long interspersed nuclear element-1 (LINE-1), which is an endogenous reverse transcriptase. Immunohistochemistry using antibody binding to LINE-1 open reading frame-1 RNA-binding protein (ORFp1) on Huh7 cells treated with BNT162b2 indicated increased nucleus distribution of LINE-1.
Significantly increased LINE-1 expression compared to control was observed at 6 h by 2.0 µg/mL BNT162b2, while lower BNT162b2 concentrations decreased LINE-1 expression at all time points
What is clear from both manufacturer and regulator documentation, including leaked supply contracts, is that there is little to no legitimate third party analysis occurring of the supplied gene therapies. This means that under those circumstances they could contain practically anything in terms of excipients or adjuvants and the only way they could be detected is through deliberate biochemical analysis, which clearly no regulator is doing. In the case of the Pfizer supply contract, a regulator or contracted recipient has only 24 hours to inspect an entire shipment. Good luck performing adequate biochemical analysis on a shipment of hundreds of thousands of doses.
Step 5
5. Effects from (2) integrated by (4) are recessive; mildly oncogenic effects in vaccine recipients unlikely to be noticed for many years
Linguistically, what this step means is that mutagenic effects (be they “manufactured genes or mutated ones) are integrated into the host genome by way of or related to LINE-1 activity. That has carcinogenic effects that are mild enough to take years to manifest to a point of detectability. Many compounds have mildly carcinogenic effects. See Monsanto’s Round Up. The rate of effect of something can also be dose dependent.
Logically and technically, I start to struggle here as I don’t understand the genetics and I’m still doubtful of the claims in Step 2 that the two mutated genes are coded for by mRNA.
Step 6
6. (5) recessive but since most of population vaccinated, in next generation female offspring have premature ovarian failure
Linguistically, this means that the hypothesised effect of introducing mutated CYP19A1 and CDKN1B genes passed from the vaccinated patient to their offspring (“recessive”), who then suffers premature ovarian failure i.e. fertility problems. By implication this may only be detected in late childhood or early adulthood in the process of sexual maturation or menstruation. Worse, it may only manifest later in the fertility or reproduction cycle.
Logically, if you achieved steps 1 - 5, it could be possible to introduce a genetic modification in the vaccinated patient which then passes to the offspring. Some of the research I’ve encountered indicates that this step is logically possible.
Technically, if one can introduce mutations into germ cells, they can be passed on to offspring. If that is done via LINE-1 activity, that has the potential to affect germ cells. Mutating CYP19A1 has effects on the ovaries and female sexual development. CDKN1B is a cancer suppression gene. Mutating it so it dysfunctions can lead to oncogenesis. Whether and how this fits directly to ovarian failure is totally unclear. Whether it would only or predominantly factor in overall mutagenic outcomes that affect the vaccinated patient directly and/or aid in the net effect on their fertility and on their offspring is an open question.
Conclusion based on the above
At this point, I’m about 60/40 in favour of this hypothesis being valid. There are detectable gaps, most obviously around step 2, which is fundamental to the whole hypothesis. I lack the technical knowledge to reject step 2, and technically I can’t be certain of any of the hypothesis.
There does appear to be a lot of circumstantial support for elements of most of the steps that, in my opinion, justifies closer scrutiny by technically capable people.
I say this because, as should now be clear, Part One discussed some of the key concepts that are at stake in this hypothesis.
If it can be proven to be essentially true, this is what it means:
The proportion of the human race who have been dosed would carry the risk of failing health, reduced lifespan, reduced fertility;
Their offspring, should they be able to have any, may be carrying defects that are undetectable by normal means at birth. Those defects are concerned with overall health via the CDKN1B gene and fertility via the CYP19A1 gene.
Now, you should fully understand why I call this the End of Hope hypothesis.
Two more points remain, which you should consider.
Date
First is the date of this hypothesis. If this was written yesterday, or in the very recent past, after much of the cited and vaccine-specific research was published, this hypothesis would in some ways be less valid because it would be easy to formulate it with existing knowledge. However, if it preceded all real-world Covid gene therapy research and data, it would raise the question of how parts of the hypothesis appear to be partially supported by research and data that were only conducted significantly after its release.
According to the source of the hypothesis that I am aware of, it was dated Wed 09 Dec, 2020. If that date is correct and not spoofed, that predates the commercial vaccine rollouts and is somewhere in the Phase 2 or initial phase 3 trials.
Credentials and source
This is the bit I’ve saved for last, for what I think is good reason.
The source of this hypothesis is an anonymous post on 4Chan.
Here is a capture of it:
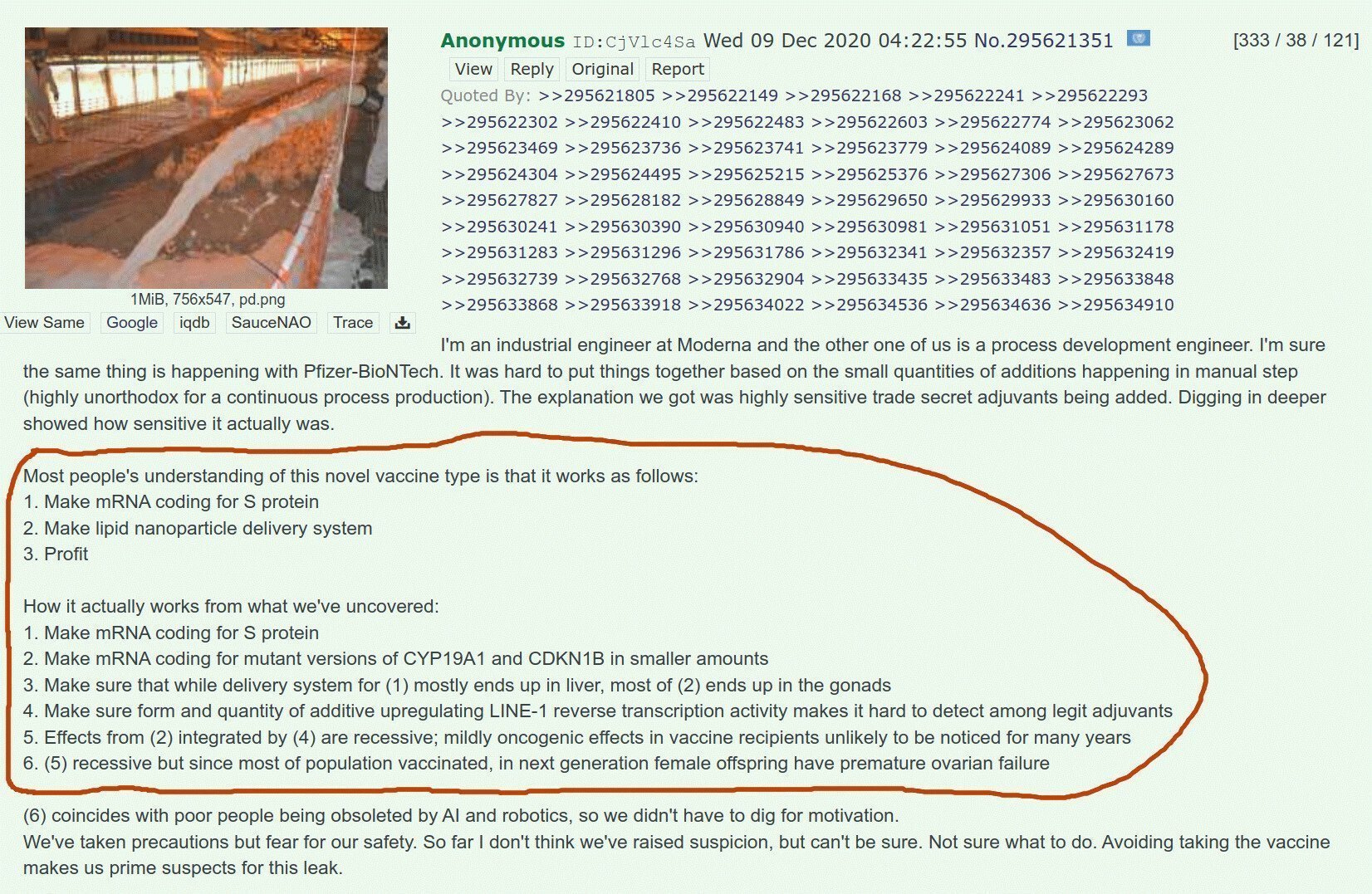
I saw this a long time ago, probably early 2021 and could not at that time process it as I didn’t have the context and knowledge to make sense of it or know whether to pay it attention. I think it has been removed from 4Chan now, but traces of it can be found on reddit and 4plebs:
https://www.reddit.com/r/conspiracy/comments/t4czx4/if_this_is_true_then_you_need_to_say_goodbye_to/
If you have not seen this before, here’s the reason why I saved the source till last. I wanted to minimise the effect of that source on any bias you, the reader have, towards processing all of the precedent information, before you made a judgement on the validity of the hypothesis.
Only you truly know what effect his final reveal has on your perception and interpretation of it.
Further, now you’ve seen the whole thing as it was posted, pay attention to the first paragraph. I’ll leave you to evaluate the whole thing in the full context of what I have presented, whether any of what I have presented supports the hypothesis’ validity and what it all means in context, if you think it could be valid.
Remember, this was published before official/mass rollout and it comes from someone who claims to be a process engineer, not a geneticist, which could explain some of the linguistic, logical and technical gaps.
Also, the first paragraph makes points about industrial production processes that when combined with the notion of real world batch variation, could be valid, given that in December 2020 there would have been much less knowledge of batch variation on a widespread basis (although manufacturers had begun mass production before roll out was authorised).
My request of you
I request you to let me know what you make of all of the above in the comments, please.
Is the hypothesis valid?
If the hypothesis is valid, does it deserve to be tested? If not, why not?
The ramifications of this hypothesis, if true, are massive.
Here is a rundown of data/evidence post Dec 2020 that backs aspects of the hypothesis:
rising all cause mortality;
declining fertility;
published negative effects on sperm volume and motility;
menstrual disturbances going as far as decidual casts, premature menstrual initiation and post menopausal menstrual bleeding;
reverse transcription;
LINE-1 activity related to the vaccines;
autoimmunity and inflammatory-based adverse events;
biodistribution characteristics;
unwillingness to conduct genotoxicity, mutagenicity and carcinogenicity tests;
excessive desire to vaccinate all people at high speed for no real benefit;
repetitive overpopulation narrative;
repetitive climate change narrative;
key players at the centre of the pandemic and vaccines who have similar positions around population and climate narratives.
Then again, it appeared on 4chan. What’s true on 4chan? It’s only the place where Hunter Biden’s cracked mobile phone contents recently appeared.
No, I am not a 4chan user. This and HB’s crack (in three senses of the word) are pretty much the only things I’ve ever visited the site for.
Good work! As an economist and non-biologist, I trust people like Spartacus, Sasha Latypova, and Kevin McKernan to out the conspiracy elements of the virus and the vaccines, which appear pretty obvious. Spartacus has another post referenced in the below about how unlikely all the alleged "coincidences" were. I intuited the hypothesis in March 2020, having taken the red pill in September 2001. The only basis for hope is supernatural, IMO. Dr. Zelenko felt the same way. cheers
https://elliottmiddleton.substack.com/p/the-theory-of-mind-and-the-current
It's striking how many doses of COVID "vaccines" are said to have been administered worldwide, around 13 billion. I'm not sure where the estimates are for how many people have had none, but I might guess between a quarter and half. I think the official estimates of the percentage "vaccinated" are intentionally too high.
In any event, 13 billion doses is huge. I wonder whether the size and speed of the campaign, and the contents of the injected products, were designed as a kind of optimum between (1) the fear that they might end up with only one good chance to accomplish some of the main goals, and (2) the effort to normalize and entrench the mRNA platform, to be used against other pathogens and for other purposes. The first of these possibilities could be described punningly as "One Shot", as Robert DeNiro says in the Deer Hunter.